Maria Hansen, MS – Final Project Update
Uncoupling Protein 2 (UCP2) is a mitochondrial protein that has been implicated in regulating the metabolic switch from glycolysis to oxidative phosphorylation (OXPHOS), which is also a key event in the functional maturation of beta-cells. In single cell sequencing studies, we determined that high levels of UCP2 expression was associated with immature stem cell derived beta-like cells (sBCs). Based on these results, we hypothesized that down-regulation of UCP2 would enhance the maturation and/or function of sBCs cells.
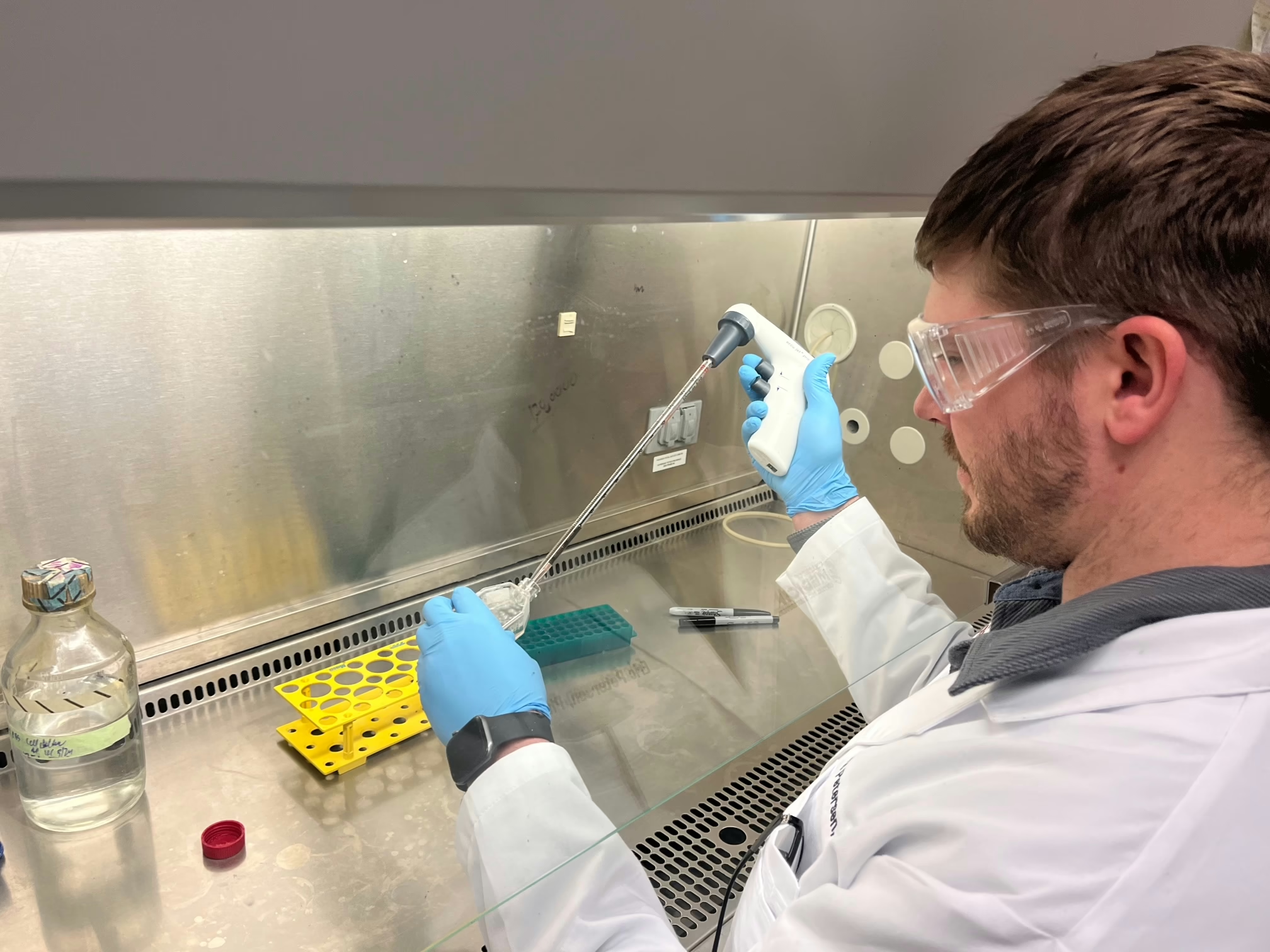
Using CRIPSR-Cas9 we generated a UCP2 knockout (UCP2KO) cell line in human embryonic stem cells. We were originally culturing UCP2KO cells in parallel with control cells using a 30-day-long beta cell differentiation protocol developed by the Hebrok lab to generate insulin-producing sBCs. Ultimately, this was giving us highly variable differentiations of both the wild type and UCP2 KO cells that made phenotypic analysis of the sBCs difficult and impeding our abilities to draw any conclusions. To address this issue, during the past six months, we have implemented a new beta cell differentiation protocol developed by the Millman lab1 that introduces much less variation between sample replicates. As a result, detecting even subtle phenotypic differences between the control and UCP2KO cell lines will be possible. Using this protocol, we are differentiating the cells in a 2D monolayer until they reach the beta-like cell stage. Next, we separate the differentiated cells into single-cells that are subsequently reaggregated to generate beta-like cell clusters. This reaggregation step purifies the population and makes us able to test the functional properties of the cells in an islet-like cluster. Our preliminary experiments, using wild type cells, have validated this as a more robust and consistent differentiation strategy.
With the optimized differentiation protocol, we are now differentiating the UCP2KO and control cells in parallel. We are utilizing a spectrum of flow cytometry panels at every major stage during the new beta cell protocol. This antibody panel includes markers against pluripotency, definitive endoderm, posterior foregut, early pancreas, endocrine specification, and immature and mature beta cells. This way, we can detect stage-specific changes in protein expression in the UCP2KO cells at a single cell resolution.
Additionally, we have recently acquired a new perfusion instrument that will allow us to perform dynamic glucose-stimulated insulin secretion assays. Using this technique, we can accurately measure insulin secretion from the wild type and UCP2KO sBCs to assess their glucose sensitivity and functional capacity.
With our improved differentiation strategy, we have begun to identify general functional differences between the control and UCP2KO sBCs. Preliminary data shows increased calcium activity at both low and high glucose levels in UCP2KO sBCs compared to controls. This matches the hyperinsulinism phenotype seen in patients with mutations in the UCP2 gene. We have also begun to assess how knockout of UCP2 disrupts sBC function and/or maturation. Finally, we are collecting samples from control and UCP2KO sBCs for RNA-sequencing. This will provide a greater understanding of the transcriptional differences between the cell populations, and it can tell us which pathways are affected by the loss of UCP2.
In summary, the UCP2KO cell line provides a model to investigate how constitutive disruption of mitochondrial function in stem cells can compromise beta cell differentiation, maturation and/or function. To also investigate dose- and time-dependent effects of UCP2 inhibition, we will perform parallel experiments using the small molecule Genipin, which has been shown to inhibit UCP2 function. Using this small molecule, we will be able to analyze the effect of UCP2 specifically at certain stages of the differentiation protocol.
1. Hogrebe NJ, Maxwell KG, Augsornworawat P, Millman JR. Generation of insulin-producing pancreatic β cells from multiple human stem cell lines. Nat Protoc. 2021;16(9):4109-4143. doi:10.1038/s41596-021-00560-y
“Every regular concern in the backcountry is doubled when you have a chronic illness. When my climbing partners run out of snacks, it’s an inconvenience. When I run out of snacks, it’s an immediate life-or-death kind of situation.”
“Sometimes I catch myself getting envious at the people around me. People who don’t carry insulin, pump supplies, CGM supplies, and a spare glucose meter in their backpack. Those who don’t have to deal with sleepless nights with clogged infusion sets, stubborn blood sugars, and constant calculations and worrying. Those who don’t have to hide catheters, tubes, and machines under their clothes. But I fight the jealousy by telling myself that I’m stronger because of it. My achievements are bigger because of it.”
“I find strength in connecting with other type 1 diabetics. Theyunderstandmy struggles with no explanation needed. And I get inspired by type 1 diabetics who climb mountains that seem impossible even to people in perfect health. They remind me that I shouldn’t let my diabetes restrict me.”
“I’m addicted to the overwhelming feeling of achievement I get from reaching a summit. It makes me push my boundaries and realize what I’m are actually capable of. Despite my chronic illness.”