
Month: August 2020
-

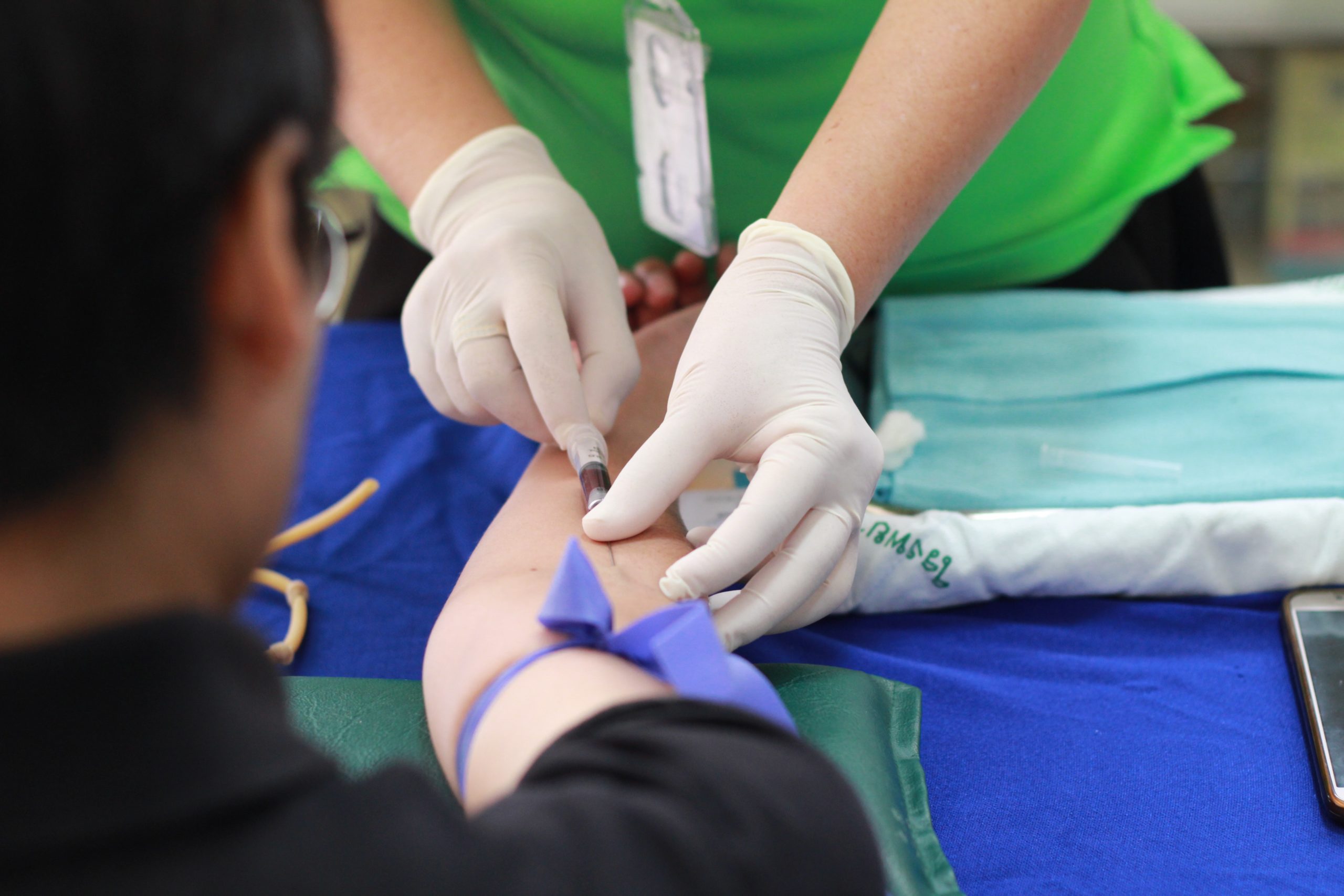
COVID-19 Symptoms in Individuals with Type 1 Diabetes
COVID-19 Testing COVID-19 has taken our country by storm, and it is affecting individuals of all ages. No one is immune, and unfortunately, individuals with underlying health conditions tend to […]
-

Protecting Insulin-Producing Islets Through Cell Editing
Protecting Insulin-Producing Islets Through Cell Editing A hallmark of type 1 diabetes is the destruction of insulin-producing beta cells in the pancreas. These cells are crucial for producing and releasing […]
-
Proactively Identifying Type 1 Diabetes
Identifying Type 1 Diabetes Development Type 1 diabetes develops when the body mistakenly attacks and destroys insulin-producing beta cells. As the number of cells depletes, the body is unable to […]
-
Helping Drive Technology Advancements
Diabetes Patients Are Helping Drive Technology Advancements Managing type 1 diabetes is an around-the-clock job. Patients must always be aware of what their blood sugar level is, whether it is […]
-

Sleep Disturbances with Type 1 Diabetes
Sleep Disturbances Common with T1D Type 1 diabetes is a disease that must be monitored around the clock. When children are awake, it is easier to tell when blood sugar […]
-

Enhancing Protection for Islets
Enhancing Protection for Islets Following Transplantation One treatment approach for type 1 diabetes that researchers have been experimenting with and refining for more than 20 years is islet transplantation. The […]
-

Reduced Out-of-Pocket Insulin Costs for Seniors Through Medicare
Out-of-Pocket Insulin Costs for Seniors The cost of buying insulin can quickly add up, but this medication is life-sustaining for individuals with type 1 diabetes. Many seniors are on a […]
-

Preserving Endogenous Insulin Production
Preserving Endogenous Insulin Production in Newly Diagnosed Type 1 Diabetes Patients A hallmark of type 1 diabetes is the body loses its ability to naturally produce enough (or any) insulin […]
-
I Believe The Mission Of The Diabetes Research Connection Is Vital!
“Entering my fourth decade of type 1 diabetes research, it is quite remarkable to look back and see how research seeking to identify answers to the questions of how this […]
-
We Need To Invest In Young Scientists
“There is a need for increased collaborative efforts to eradicate diabetes. We need to invest in young scientists with new and fresh ideas that are willing to dedicate their career […]
-

Advancing Efforts of Early-Career Scientists
“The Diabetes Research Connection will advance the efforts of early-career scientists whose innovative proposals for diabetes investigations might be overlooked by government funding agencies in favor of more conventional research.” […]
-

We select the research we believe in!
“We support the Diabetes Research Connection because it affords us the rare opportunity to select the research that we believe in and to better understand it by interacting with the […]